
GBD 2023 – Intimate partner violence and sexual violence against children
Published December 16, 2025
Sexual violence against children and intimate partner violence against women are two of the most devastating yet persistently underrecognized global health challenges and rank among the top risks for mortality and morbidity worldwide, according to research published in The Lancet.
This video shares key findings from this study.
Video transcript
This transcript has been lightly edited for clarity
Violence against women and violence against children represent two devastating, yet underrecognized, global health challenges. A new analysis in the Global Burden of Disease (GBD) 2023 seeks to address this by estimating the prevalence and attributable disease burden of intimate partner violence (IPV) among females and sexual violence against children (SVAC) among males and females.
IPV and SVAC are not just social problems, but two of the world’s most critical public health issues, the fourth- and fifth-leading risk factors for DALYs among young women worldwide. More than 1 billion people have experienced SVAC, and more than 600 million women have experienced IPV, leading to wide-ranging health problems like major depressive disorder, HIV/AIDS, and self-harm.
For the first time, the GBD study has comprehensively mapped a broad range of health outcomes to these forms of violence, revealing a burden far greater than we previously realized.
So, let’s explore the latest paper from GBD 2023, “Disease burden attributable to intimate partner violence against females and sexual violence against children in 204 countries and territories, 1990–2023,” for more detail.
First off, we define IPV as “the lifetime experience of at least one act of physical or sexual violence by a current or former intimate partner since the age of 15, among females.”
And we define SVAC as “the lifetime prevalence of intercourse or other sexual contact (i.e., fondling and other sexual touching) before the age of 18, where the contact was unwanted (i.e., physically forced or coerced)” among both males and females.
To link IPV and SVAC to disease burden, we made three major sets of estimates:
First, we estimated how common these forms of violence are (prevalence).
Then, we measured the relationship between these forms of violence and health outcomes (relative risk).
Finally, we calculated the PAFs, DALYs, and deaths attributed to each risk factor.
To make these estimates, we identify data, adjust that data, and then use modeling tools to make estimates. Here’s how it works:
As we said, the first step was to estimate the prevalence of IPV and SVAC.
To do this, we identified data from household surveys—specifically those that asked about violence against children and women. We focused on self-reported data from nationally or subnationally representative surveys. And ultimately, we found 594 sources on IPV and 460 sources on SVAC.
Because surveys use different definitions of IPV and SVAC, we had to standardize data using several adjustments. For example, using a tool called MR-BRT, we adjusted for differences in reporting, like “past year” vs. “lifetime” exposure. For SVAC, confidential self-reports disclosed more cases than face-to-face interviews. To account for this difference, we used linear regression to adjust data from traditional interviews to more closely match confidential self-reported levels. We also split broad age groups into five‑year age groups.
After adjusting the data for various differences, we estimated the prevalence of IPV and SVAC using a model called spatiotemporal Gaussian process regression (or ST-GPR). ST‑GPR uses models and borrows strength across time, locations, and age to produce consistent prevalence estimates, even for locations with no direct data.
Next, we estimated relative risk. To do this, we needed to find evidence linking these forms of violence to specific health outcomes. We conducted a systematic review of scientific literature published between 1970 and 2024. In this review, we searched seven different databases, screened over 75,000 potential studies, and ultimately found 36 studies on the health outcomes of IPV and 114 studies on SVAC we could use.
For both risk factors, we analyzed the relationship between violence and each health outcome using the Burden of Proof, a meta-analytical approach that synthesizes and evaluates the strength of existing evidence. We carried out these analyses for risk-outcome pairs with at least three studies from our systematic review. This allowed us to explore associations with IPV and SVAC that had not been examined in the GBD before. Only associations with meaningful statistical relationships are included in our results.
In the end, we expanded the list of health outcomes linked to both IPV and SVAC in GBD 2023, with eight outcomes linked to IPV and 14 linked to SVAC. These include mental health disorders such as major depressive disorder, as well as diseases like type 2 diabetes and HIV/AIDS, and injuries, such as interpersonal violence and self-harm.
You can explore each risk-outcome pair, and estimated relative risks, in our Burden of Proof visualization tool online.
In the last step, we used prevalence estimates and relative risks to calculate population attributable fractions (PAFs). PAFs tell you the proportion of a disease that is caused by a specific risk factor.
We then use these PAFs, along with disease-specific estimates from GBD 2023, to figure out how many DALYs and deaths could be prevented by eliminating all cases of IPV and SVAC.
Let’s take a look at what we found in this analysis. The numbers are staggering.
In 2023, 608 million females aged 15 and older experienced IPV during their lifetime, contributing to 145,000 deaths.
The SVAC is equally devastating: an estimated 1.01 billion people aged 15 and older experienced sexual violence during childhood, contributing to 290,000 deaths among males and females in 2023.
The prevalence of IPV and SVAC is high everywhere, with large differences across countries. Looking at this map of IPV prevalence, we can see countries across many regions with prevalence of 20–30%, and some of the highest rates in sub-Saharan Africa, South Asia, Southeast Asia, East Asia, and Oceania.
The highest rates of SVAC are also in South Asia and sub-Saharan Africa, followed by the high-income region.
When compared to other risk factors, these two risk factors are major drivers of global disease burden, especially for young and middle-aged adults.
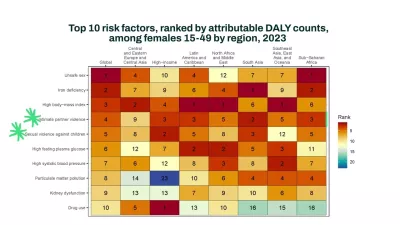
For females aged 15–49, IPV was the fourth- and SVAC was the fifth-leading risk factor for DALYs in 2023. Looking at this figure, we can see that these are major risk factors across all regions of the world, outranking many widely recognized health threats, like high fasting plasma glucose or high blood pressure. For males 15–59, SVAC was the 11th-leading risk factor for DALYs.
For IPV, the leading causes of health loss were anxiety disorders and major depressive disorder. These are the blue causes in this figure.
As you can see, there are substantial differences in different regions of the world, with the global estimates on the far left. In sub-Saharan Africa, HIV/AIDS is the leading cause of health loss associated with IPV, while in high-income countries, drug use disorders are a stand-out cause.
SVAC and health outcomes
Now, let’s look at the causes associated with SVAC. SVAC is linked to 14 health outcomes. Mental health disorders, in blue, contributed most to lost years of healthy life. These include schizophrenia, major depressive disorder, and other mental health conditions.
Like IPV, there are major differences across regions and some differences across sex as well. In South Asia, self-harm, in green, is a notable health outcome for SVAC. Substance use disorders, in orange, are particularly high in high-income locations.
Summary of results
So, to recap what we’ve covered, GBD 2023 greatly expands our understanding of the disease burden caused by intimate partner violence and sexual violence against children.
More than 600 million females 15 and older have experienced intimate partner violence. More than a billion people 15 and older have experienced sexual violence as children.
New evidence links IPV and SVAC to a wider spectrum of health outcomes than previously recognized. IPV and SVAC rank in the top five health threats globally for women aged 15–49.
IPV contributes significantly to healthy life lost among women due to anxiety, self-harm, and interpersonal violence (injuries and homicide). SVAC is a major driver of the overall burden of mental health conditions, self-harm, and drug use disorders.
Despite these estimates, IPV and SVAC are probably underestimated due to stigma and underreporting. Their true impact is probably even greater.
Data on sexual violence is complicated. Many survivors don’t report their experiences because of stigma. In some regions of the world, surveys about these risk factors are missing or incomplete. Sometimes adults are asked to remember childhood experiences, which can be unreliable. And people’s willingness to share has changed over time, making comparisons harder.
Also, definitions aren’t consistent. Different studies measure violence in different ways, using different timeframes and methods. Some forms of violence, like psychological abuse, are missing from this analysis because there’s no global agreement on how to measure them.
We need more high-quality cohort studies to better understand the link between violence and long-term health outcomes. The picture is incomplete, and more attention and investment are needed to both measure and address this global health crisis.
Investing in comprehensive and coordinated prevention and support has the potential to avert millions of DALYs every year. Violence is a massive, avoidable risk factor, one of the world’s most significant drivers of disease and disability. Intimate partner violence and sexual violence against children are not only criminal and social justice issues, but major public health emergencies as well.
These forms of violence should be public health priorities, to prevent violence, support survivors, and ultimately reduce global disability and premature mortality.
For more details on our results, including more results by age, sex, and location, check out the paper in The Lancet, or explore them yourself on GBD Compare and the Burden of Proof tool.