
Vaccine coverage
Vaccines are a powerful tool for saving lives and improving health, but their power can be diluted by gaps in coverage. We study routine childhood immunizations to understand and address these gaps.
Photo by Heather Hazzan for SELF magazine, Flickr.
Access our vaccine coverage estimates
At IHME, we gather comprehensive data on vaccination coverage and use statistical models to estimate vaccine coverage at global, national, and local levels, with the goal of providing better evidence to guide critical decisions about vaccine policy. All of our estimates are updated regularly and are publicly available.
- Download: Use our data portal to download our estimates of vaccine coverage.
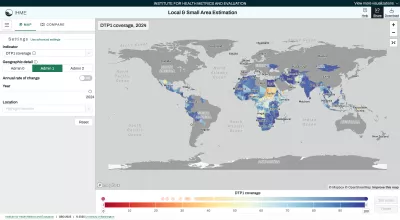
- Interact: Explore local coverage estimates in our interactive visualization tool.
Global Burden of Disease (GBD) study
For the GBD study, we also estimate the burden of vaccine-preventable diseases by age, sex, location, and over time. These estimates can be explored in GBD Compare and through the GBD Results tool.
Collaborate with us
We work closely with partners around the world and the GBD Collaborator Network to make sure that our estimates are as accurate and useful as possible. If you’re interested in collaborating, please contact us at [email protected].
About our vaccine coverage work
We define vaccine coverage as the proportion of children who received at least the stated number of doses of each vaccine during the year that cohort was of the target age of vaccination. For example, DTP3 coverage in 2010 represents the proportion of children under age 12 months in 2010 who received at least three doses of a diphtheria-tetanus-pertussis-containing vaccine.
For our routine coverage estimates, we exclude campaign doses when possible. For some vaccines (e.g., measles), we additionally estimate age-specific vaccination coverage and combined coverage (from both routine immunization services and vaccination campaigns). When using survey data, we consider children to be vaccinated if they have valid doses recorded on a home-based record (“card doses”) or if their parents report that they have been vaccinated (“recall doses”).
We estimate multiple vaccines at the global, national, regional, and local levels in a comprehensive framework so all our estimates can be compared consistently between places and over time.
- Diphtheria-tetanus-pertussis (DTP)
- Measles-containing vaccines (MCV)
- Haemophilus influenzae type B (Hib)
- Rotavirus (Rota)
- Pneumococcal conjugate vaccine (PCV)
- Hepatitis B (HepB)
- Polio
- Rubella (RCV)
- Bacille Calmette-Guérin (BCG)
Vaccines are one of the most important public health success stories in history, and the resurgence of vaccine-preventable diseases anywhere is a threat to all of us, everywhere. The challenges and barriers leading to the failure to immunize vary broadly from country to country and community to community, meaning that contextually tailored and locally informed solutions are required. Tracking progress and identifying both successes and gaps in coverage—both between and within countries—is a vital first step toward achieving complete and equitable coverage for all people around the world.
Our research methods are described in detail in our peer-reviewed scientific publications, which can be found in the research library.
Funding for this work was provided by the Bill & Melinda Gates Foundation and Gavi, the Vaccine Alliance.
Our data sources include both survey data and administrative data, recorded in the Nextcloud folder and our data catalog, the Global Health Data Exchange (GHDx).
- Survey data includes the Demographics and Health Survey and others.
- Administrative data refers to official data reported by countries to WHO.
We check for data quality issues before running our models both by analyzing the data and by looking at external sources of information about the data. Where possible, we use statistical techniques to quantify and adjust for biases in the data – for instance, we adjust for the difference between survey data and official country-reported data.
- Excluding data: In some cases, when there are significant concerns about data quality, those sources may be excluded from the models. Our models use trends in time and predictive covariates to produce estimates of vaccine coverage for locations and years in which no data are available.
- Predicting uncertainty: We also produce estimates of the uncertainty for our predictions – when data are sparse or conflicting, our estimates are more uncertain.
- Advocating for data quality: While these models provide valuable insights into vaccination coverage in settings where data are missing or of lower quality, they aren’t a replacement for high-quality data. We support the broader efforts of the immunization community to strengthen data quality.
